

By: Ryn Williams, Social Media Manager
Near the start of the pandemic, the Center for Disease Control and Prevention (CDC) announced that blue lips are a possible symptom of COVID-19. Medically, this is referred to as “cyanosis,” and it happens when the body doesn’t receive enough oxygenated blood.
It is ignorant to assume that symptoms appear the same way for people of all races – in Black people, cyanosis is more likely to appear in the gums than in the lips, meaning that their symptom may go unnoticed by a white doctor.
This is not the only case of irresponsible disparity in medicine. Since the 1700s, and likely before that, there have been myths that Black patients are simply less sensitive to pain, that Black people’s skin is thicker than white people’s skin, that Black people are stronger than white people, and so on.
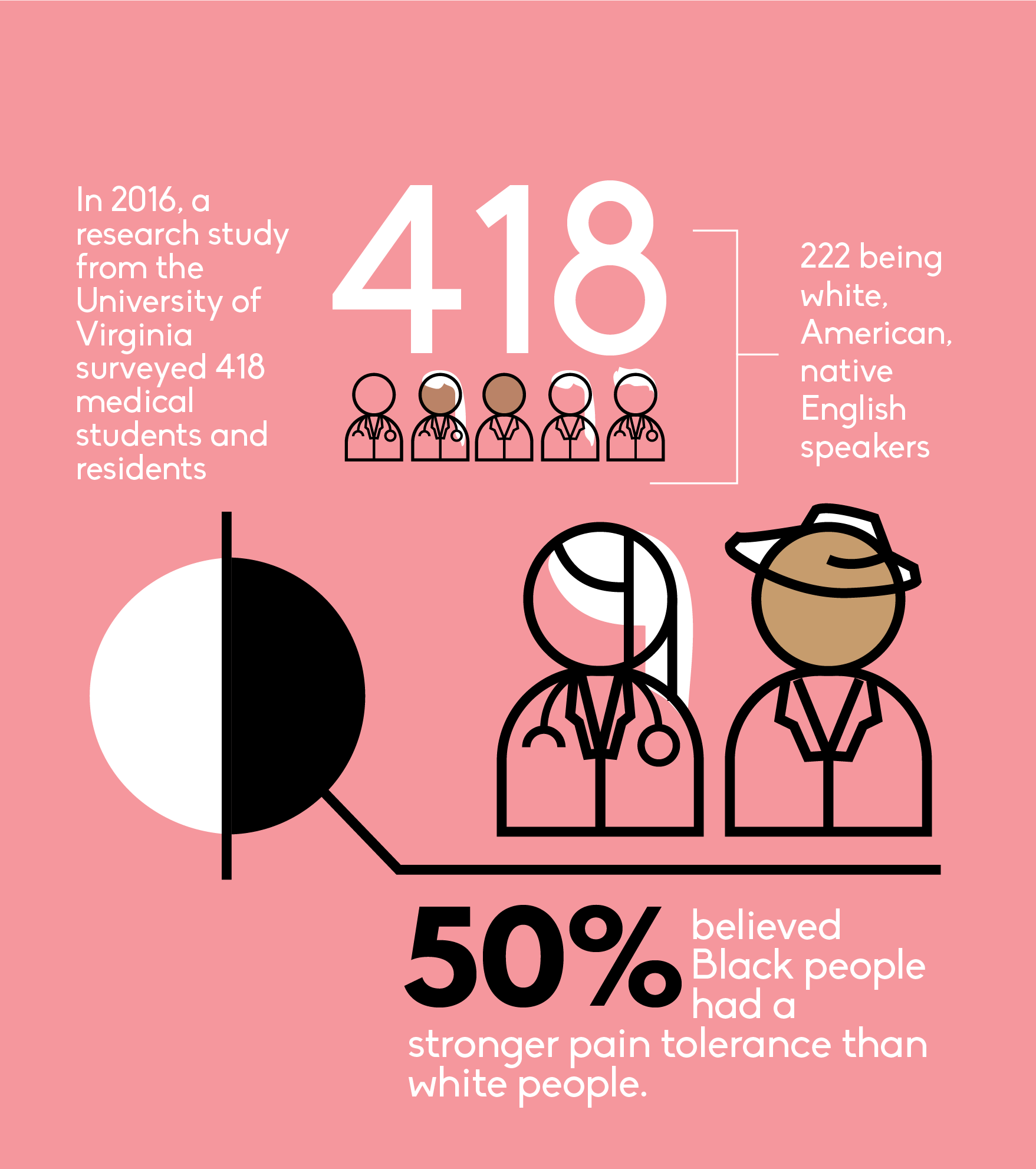
In 2016, a research study from the University of Virginia surveyed 418 medical students and residents (with 222 being white, American, native English speakers) and found that 50 percent of them believed Black people had a stronger pain tolerance than white people.
This carelessness leads to events like four-time Olympic gold medalist Serena Williams’ life-threatening experience giving birth to her daughter at St. Mary’s Medical Center in West Palm Beach, Florida. She experienced pulmonary embolism, and due to her history with it, was able to identify it immediately.
Shortly after giving birth, Williams walked out of her own hospital room and insisted to a nurse that she needed a CT scan and an IV heparin,a blood thinner. The nurse assumed that her pain medication was causing her to be confused. When Williams finally convinced a doctor to perform a CT scan, they realized several blood clots were forming on her lungs.
Had the nurse ushered her back to her room, she may have died.
“Even Serena Williams can’t get proper care,” Britt Julious, a music critic for the Chicago Tribune, tweeted in response. “This is why black [sic]women are statistically at the greatest risk for pregnancy-related deaths. The medical community does not take our pain seriously.”

In the modern world, the United States is an outlier: women are more likely to die from childbirth and pregnancy related causes here than anywhere else. In the U.S., Black women of all incomes are three-to-four times more likely to die from pregnancy complications than white women, the CDC states. Research suggests that almost half of these deaths are preventable.
California seems to be the only state to care. Forming the California Maternal Quality Care Collaborative (CMQCC) in 2006, they were determined to understand and stop maternal mortality. Due to their efforts, they have managed to reduce maternal mortality rate in women from 16.9 per 100,000 people to 7.3.

The CMQCC has been working closely with organizations led by Black women, but there is still work to be done to end racism in the healthcare industry.
A 2016 study published in the Journal of Clinical Oncology found that Black women were less likely to undergo testing for BRCA1/2, a gene that determines breast and ovarian cancer risk, than white women. Black women were less likely to report that they received any physician recommendation for testing even if they showed signs that they were at-risk for it. There is no medical basis for this discrimination: the probability of carrying the BRCA1/2 mutation is similar between both races.
Racial segregation still exists in the U.S., and it thrives in hospitals.
Schedule II opioids sit in time-locked safes in pharmacies all around the U.S. These drugs can be prescribed either for long-term pain management, or three-day supplies in the wake of a car accident.
Black Americans are two times less likely to receive opioid prescriptions than white Americans, but their pain is the same. Doctors have been found to be overly cautious when prescribing to Black patients, and this is likely due to stereotypes of what an opioid addict looks like – which harms both Black and white patients.
This discrimination begins at birth, as Black newborns are more than twice as likely to die than non-Hispanic, white newborns. It doesn’t end there.
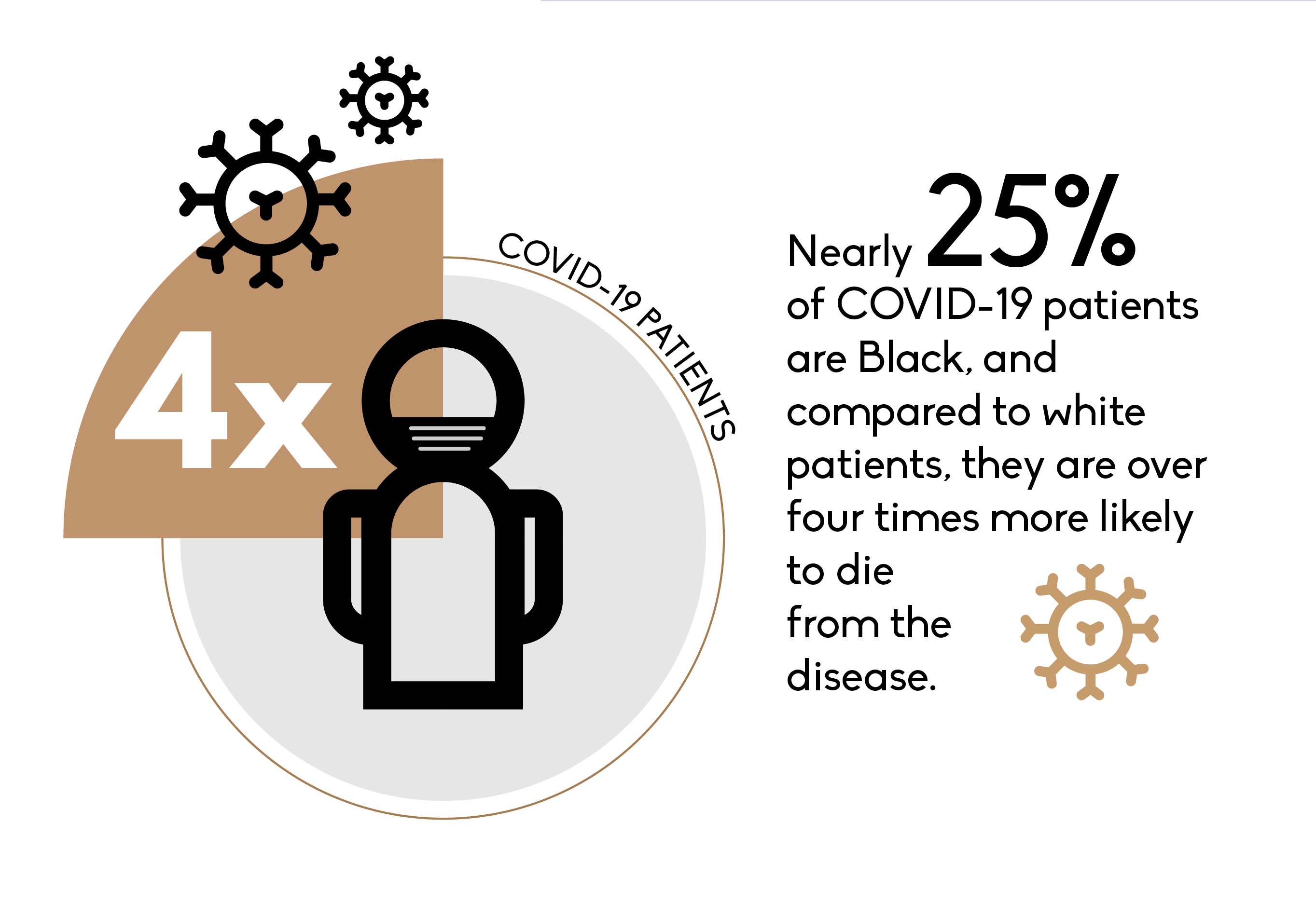
Nearly 25 percent of COVID-19 patients are Black, and compared to white patients, they are over four times more likely to die from the disease.
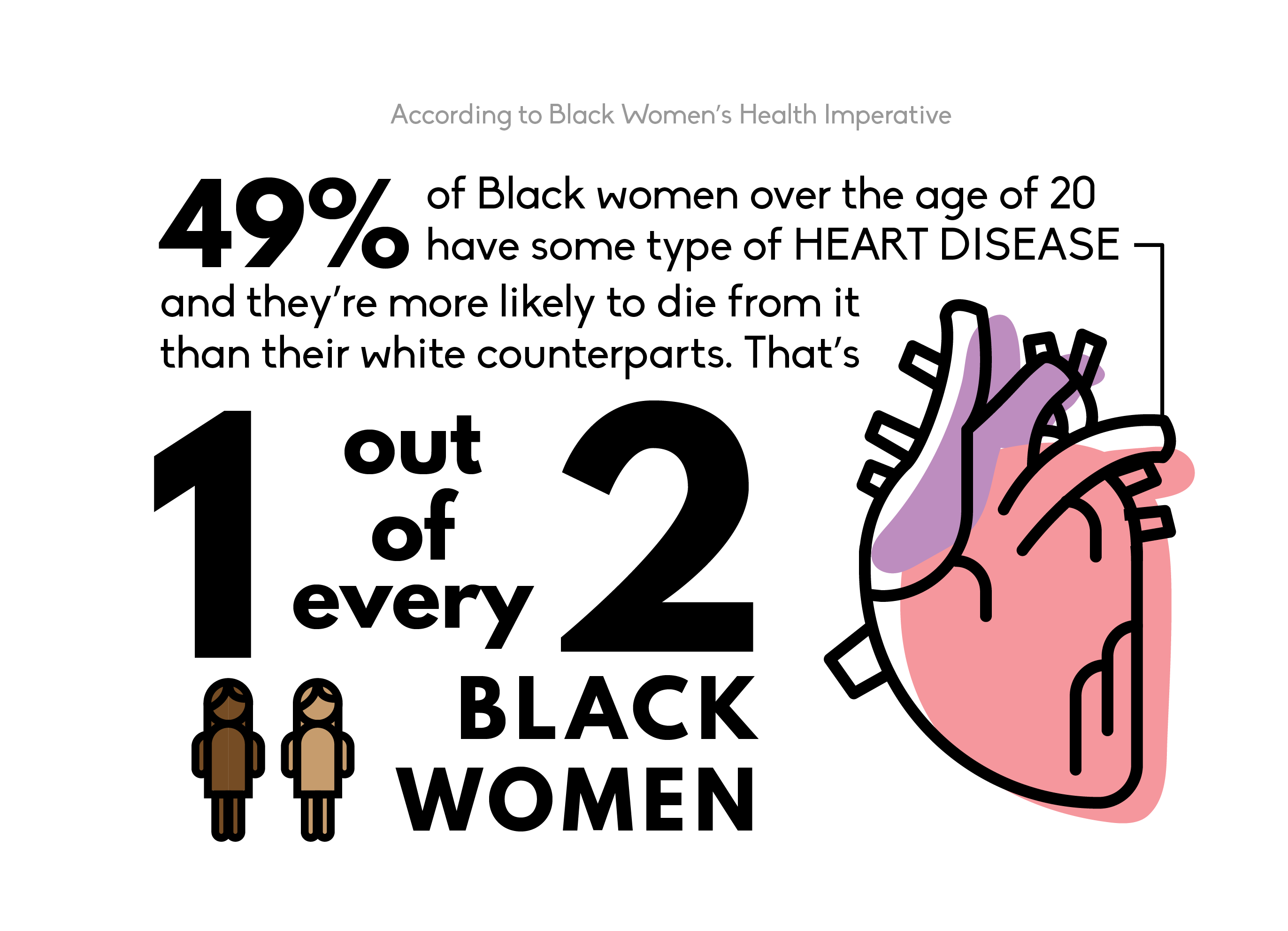
49 percent of Black women over the age of 20 have some type of heart disease, according to Black Women’s Health Imperative, and they’re more likely to die from it than their white counterparts. That’s one out of every two Black women.
There are a few causes for this. Negligent testing is one of them, along with preexisting conditions like obesity, which affects 82 percent of Black women, and diabetes, which affects 25 percent of Black women over the age of 55. On average, one in five Black women smoke cigarettes, another contributor to the heart disease epidemic.
Fortunately, there have been efforts to curb the risk of heart disease in the Black community. The Truth Initiative, a campaign to prevent tobacco usage in young Americans, published a video last year bringing attention to tobacco companies predatory advertisements to Black communities.
Black women are the demographic that suffers the most from heart disease out of all Americans. Despite that statistic, no major heart health organizations have pushed statements for Black women specifically or individually.
Nearly sixty years ago, Malcolm X announced, “The most disrespected person in America is the Black woman. The most unprotected person in America is the Black woman. The most neglected person in America is the Black woman.” He was right.



